Designing for trust in predictive prevention
An exploratory project for Public Health England by Projects by IF.
What was it?
Public Health England (PHE) was investigating how they may be able to implement what they called "preventative care". They wanted to combine public health datasets with lifestyle data from people's phones. By doing so, they could make interventions at key moments (when buying food, when deciding routes to work, etc.) to improve the person's health and help prevent certain diseases, such as type-2 diabetes and certain types of asthma.
However, they were concerned with how they might do this without betraying public trust. What design language could they use? How might they structure their data policies? What language should they communicate with?
Timeline and roles
Project timeline: 6 weeks
My responsibilities:
- Design leadership
- Digital and paper prototyping
- User and desk research
- Insights compilation and strategic recommendations
Team composition:
- 1 project lead
- 1 strategy
- 3 design (service, graphic)
- Additional support from subject matter experts in data rights, privacy, and data architecture
Project timeline
Research
Phase 1
Desk research, interviews, and knowledge capture.
Prototype and test
Phase 2
Prototyping. Testing with users, sense-checking and additional interviews with experts.
Insights & strategy
Phase 3
Testing and insights result. Recommendation generations. Strategic recommendation. Delivery.

Research
Both PHE and Projects by IF came to this project with a huge amount of pre-existing knowledge. We reviewed the ongoing and pre-existing projects and interviewed key experts and stakeholders.
These interviews flagged:
- There was no proven use-case for this kind of health prevention
- Without a plan for how the data will be used, informed consent will be impossible
- Responsibility for data sharing should be more than the individuals
Right: Research and interviews done at the PHE offices in London.
Prototype and test
While the interviews outlined the public health and medical concerns around predictive prevention, they did little to understand public trust.
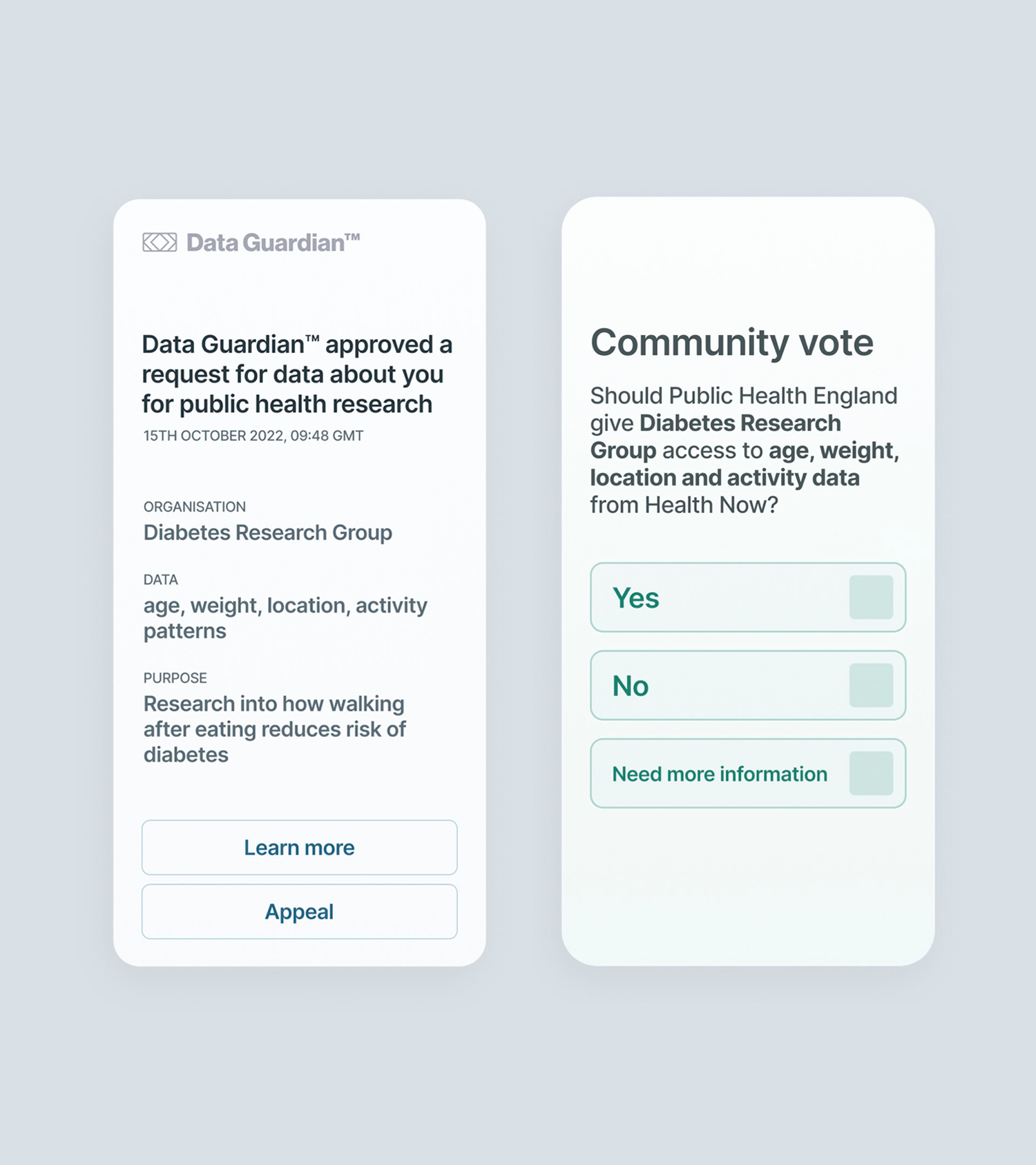
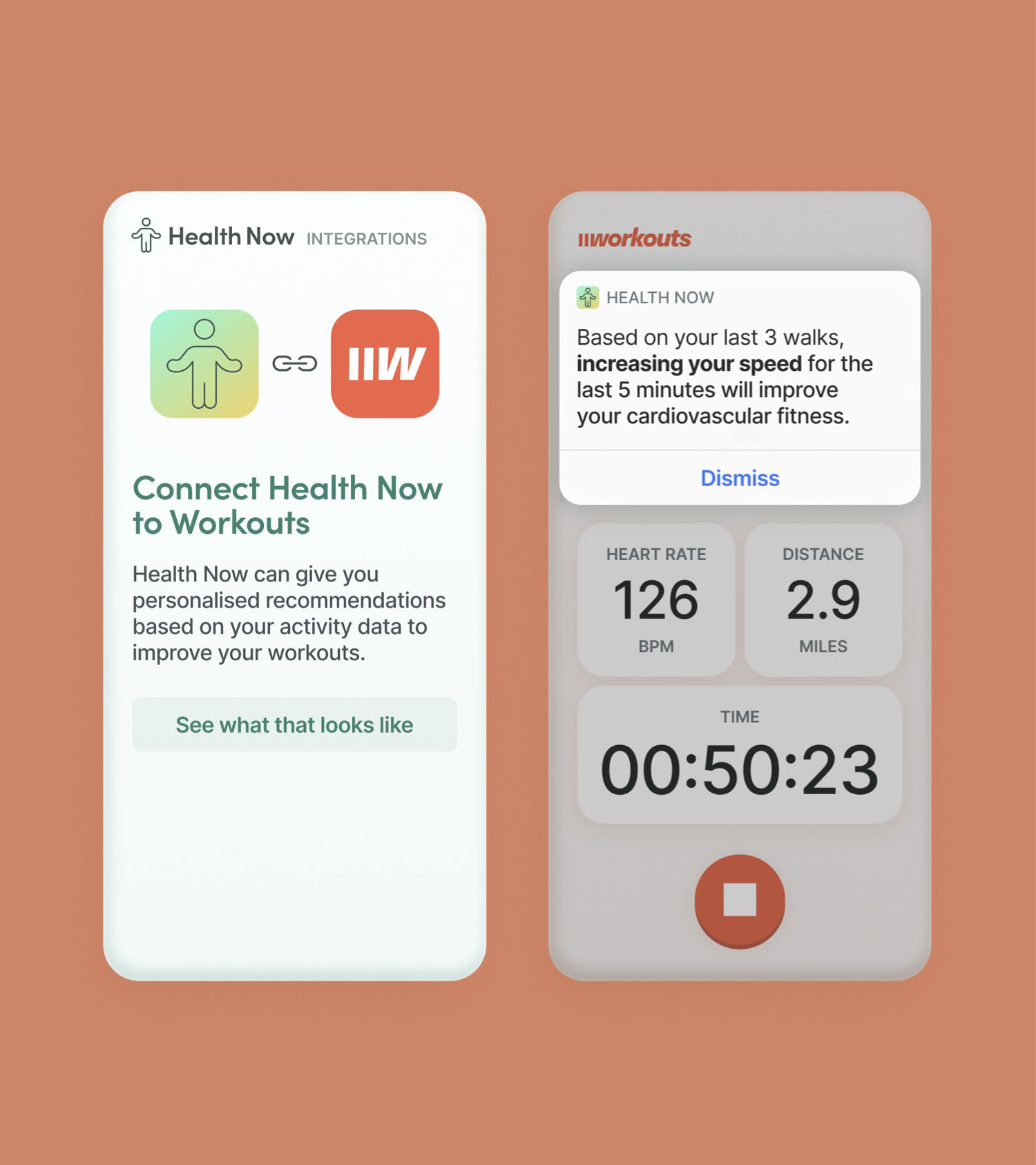
So, we prototyped and tested a number of mock-ups and flows. They investigated various methods in the experience flow: from how things would be communicated to how 'invasive' the functionality could be.
Left: Paper mock-ups used for testing. Purposely made in a very low fidelity, sketched style for better testing results.
Phase 3: Insight generation and delivery
The desk research and user testing generated a lot of data and opinions — some of which contradictory. We combined this with our pre-existing knowledge of trust in data to create key design insights and strategic next steps for PHE.
User-research outcomes
The testing made clear some basic principles to help guide the future investigation of trust and consent with users:
- Start small with data collection. The least amount possible.
- Show impact of data sharing in-context of the sharing moment.
- Add friction to key moments.
- Make consent prominent.
- Show PHE can he trustworthy, early, before asking to collect data
Where user research failed
One thing explored in the testing sessions with the public was about their knowledge of the information on their phone, public health datasets, and the impacts of combining them.
It was clear that people had mixed — and sometimes inaccurate — perspectives on what it means to combine data and what the benefits and harms of doing so would be.
This highlighted a massive problem with traditional user-testing, as understanding impacts, risks, and benefits of data sharing with respect to public health.
We recommended continuing research and investigation in a societally-aware way.